A Discussion of Tripping Over the Truth…
By Carl Nelson
A Discussion of Tripping Over the Truth/ How the Metabolic Theory of Cancer Is Overturning One of Medicine’s Most Entrenched Paradigms – by Travis Christofferson, MS
 “Cancer therapy could be a gentle rehabilitation.” (Pg. 185)
“Cancer therapy could be a gentle rehabilitation.” (Pg. 185)
“In a 2004 Fortune article entitled “Why We’re Losing the War on Cancer,” author Clifton Leaf wrote: It is already the biggest killer of those under 75. Among those ages 45 to 64, cancer is responsible for more deaths than the next three causes – heart disease, accidents, and stroke – put together. It is also the leading killer of children, thirtysomethings – and everyone in between.”
In short, in the words of Arlo Guthrie regarding his Vietnam-day collision with the draft: “…the only reason I’m singing you this song now is cause you may know somebody in a similar situation, or you may be in a similar situation…[There is a near certainty that either you, (or someone you love), will be diagnosed with a cancer in this lifetime.] …and if you’re in a situation like that there’s only one thing you can do…”
And it’s probably not to start singing to the doctor the refrain to Alice’s Restaurant – though perhaps apropos. Because like Vietnam, you will getting shipped off to a war not of your choosing, led by leaders you might not choose (if you’d known).
To “slash and burn”, (surgery and radiation), has been added “poison” (chemotherapeutics) to the physicians’ cabinet of tortures since cancer’s first appearance centuries past.
“Science writer Ralph Moss noticed the odd criteria that the FDA used to approve drugs that allowed scores of ineffectual drugs to gain control: “If you can shrink the tumor 50 percent or more for 28 days you have got the FDA’s definition of an active drug. That is called a response rate, so you have a response… [but] when you look to see if there is any life prolongation from taking this treatment what you find is all kinds of hocus pocus and song and dance about the disease free survival, and this and that. In the end there is no proof that chemotherapy in the vast majority of cases actually extends life, and this is the GREAT LIE about chemotherapy, that somehow there is a correlation between shrinking a tumor and extending the life of the patient.” (Quoted material is from the discussed book.)
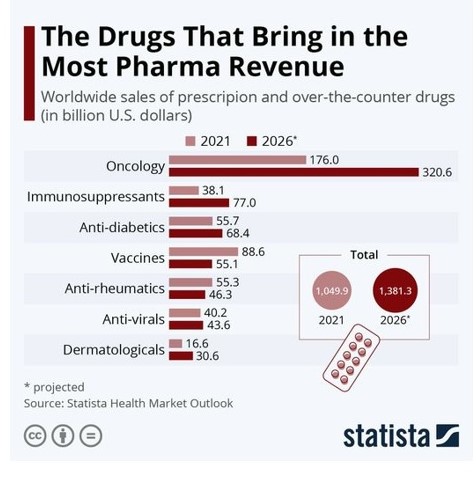
So why is it done? This bar graph might hide a large portion of the answer in plain sight:
 “An example of the current state of cancer drugs is bevacizumab (Avastin). It received FDA approval in 2004 for the treatment of metastatic colon cancer and later received approval for other applications including breast cancer. To treat the average breast cancer patient with bevacizumab cost $90,816 per year without extending overall survival. But because it shrank tumors in a fraction of cases, the FDA approved it, highlighting the absurd criteria used for drug approval. Worse, patients who were treated with bevacizumab on top of paclitaxel had double the chance of experiencing significantly higher toxicity. Doctors must have realized the contradiction when recommending bevacizumab. Did they really tell patients that they should take a full course of the drug but would likely experience two and a half times the normal toxicity? The drug cost almost $100,000 and wouldn’t extend life at all. Why would an oncologist prescribe it? “There is a shocking disparity between value and price, and it’s not sustainable,” said Roy Vagelos, MD, at the 2008 annual meeting of the International Society for Medical Publication Professionals.
“An example of the current state of cancer drugs is bevacizumab (Avastin). It received FDA approval in 2004 for the treatment of metastatic colon cancer and later received approval for other applications including breast cancer. To treat the average breast cancer patient with bevacizumab cost $90,816 per year without extending overall survival. But because it shrank tumors in a fraction of cases, the FDA approved it, highlighting the absurd criteria used for drug approval. Worse, patients who were treated with bevacizumab on top of paclitaxel had double the chance of experiencing significantly higher toxicity. Doctors must have realized the contradiction when recommending bevacizumab. Did they really tell patients that they should take a full course of the drug but would likely experience two and a half times the normal toxicity? The drug cost almost $100,000 and wouldn’t extend life at all. Why would an oncologist prescribe it? “There is a shocking disparity between value and price, and it’s not sustainable,” said Roy Vagelos, MD, at the 2008 annual meeting of the International Society for Medical Publication Professionals.
The cost benefit relationship for almost every one of these drugs was marginal at best and nonexistent at worst. The cost for cancer drugs went from an average pre -reatment course of about $5,000 before 2000 to $40,000 by 2005, and in 2012 almost every new drug was priced at more than $100,000 in the United States. The United States spent twice as much as any other country on oncology and medical care in general yet achieved the same survival rate except for breast cancer and lymphoma, where it eked out a 1 to 2 percent improvement.” (Pg 13-131)
And now that I may have your attention, I will say something about the book:
Tripping Over the Truth is riveting reading. Well written and expertly plotted as non-fiction can be, the science writer, Travis Christofferson MS, has turned in a gem, which could also prevent financial loss, terrible suffering and perhaps save the life of yourself or that of someone you know.
The book starts in 1924 with a brilliant German chemist, Otto Warburg, making a claim that cancer was basically a disease of damaged cellular metabolism. This was after follow-up investigations of his finding that a definitive marker of cancerous cells was that they all produced their energy through anaerobic respiration. “Unlike normal cells,” Warburg found, “cancer cells ferment glucose in the presence of oxygen, a characteristic now known simply as “the Warburg effect”. (Pg 16) (Normal cells use aerobic respiration – resorting only to the less efficient anaerobic processes when adequate oxygen is not forthcoming (such as during extreme exercise).
Warburg’s ideas gradually fell from fashion as the attentions of the newer generations were drawn towards other enticing observations, the first of which involved causative cancer agents, after the initial observation by a London Surgeon, Percivall Pott, that young chimney sweeps were prone to scrotal cancers. Other observations hung on the damaged nature of the nuclear chromosomes of cancer cells, also their lack of cellular differentiation. And infectious nature was speculated upon when it was found that transferring a tumor from a chicken could create like cancer in another. That cancer was a product of mutations to the genetic coding of a cell became a most popular and funded possibility of the latter twentieth century. But by the time a complete transcription of the human genetic code was finally achieved, it was becoming clear that if mutations were the cause of cancer, then likely the cure was not to be in our purview: the suspects were far too numerous and actions elusive. “The bewildering degree of intertumoral heterogeneity did not allow the origin of any type of cancer to be conclusively assigned to a specific set of mutations. It painted cancer as a disease that changed the rules on a whim, a capricious monster that played outside the realm of cause and effect.” (Pg. 120
It is at this point where focus once again turned on to the more positive results of isolated labs whose work had continued to elaborate on the findings of Otto Warburg, which pointed to a single-sourced explanation for a dispersion of catastrophic effects. To this recipe, add human nature:
“Nothing is perfect. Life is messy. Relationships are complex. Outcomes are uncertain. People are irrational” – Hugh Mackay, social researcher, (Pg. 197)
And you have all of what’s needed for a gripping detective yarn.
If you have an MD, like myself, and are familiar enough with medicine and its terms, and enough cellular physiology to be fairly comfortable reading substacks by MDs and researchers – you will eventually have sorted enough wheat from the chaff to follow the kernels of truth to their generally credible source. It’s in the search wherein most of the credibility of the conclusion is acquired. Unfortunately, like a whale, when you surface – seemingly to others, from out of nowhere to spout some revealed truth through your blowhole – your others, who haven’t made this intellectual journey, often find what you have to tell them so urgently, strikes them as querulous, as they haven’t heard anything of even a like sort mentioned. At worse, they might view you as a harmful person – maybe go so far as to be a demon who is attempting to undercut what has been accepted by all the experts to be beneficial – and thereby hurting people with your views.
I don’t practice, never have, but you might imagine the damping effect this attitude has upon the practicing physician who decides to look into matters for himself. First, this rarely happens as the practicing physician is far too busy treating patients to track treatment rationales to their origins. In order to stay current, they commonly subscribe to a service which provides physicians with the latest research and regarding diseases and their treatments. My own doctor gave me the website he uses. I had a look. The top entry was regarding the new schedule for Covid vaccinations involving children.
The thing about doctors is that they are “trained”.
“…as medical students… The medical curriculum is so overloaded with information what you just have to learn what you hear, as you hear it…” – Dr. Donegan in his Foreword to Dissolving Allusions by Suzanne Humphries, MD
Very little time is allowed for questioning. (You might be interested to read of my own ‘sabbatical’, “Flaneur / A Memoir” )
And these medical students become doctors who are like the robotic arms of the current medical establishment, which creates the “Accepted Standard of Care” for various medical conditions. To practice outside of the accepted care standard risks lawsuits, and disciplinary action (including the loss of the license to practice). Basically, you may kill people safely within the accepted care standard, but if you are saving lives willy-nilly in any manner outside of the standard of care, all of the above lawsuits and disciplinary actions might very well occur to you – and not because anything untoward which you, the physician, might have caused. Someone along the line or in the medical chain of command might have taken umbrage, and the physician’s professional life could very well be over.
For these reasons it is very hard oftentimes for researchers to convince physicians to try out new treatments on patients – even for very promising therapies offered to clinically hopeless patients’ cases. This is also the reason many much more effective therapies than those commonly practiced remain unknown, because the physicians will not publish their – even very positive – findings for fear of retribution.
Another reason you might not see very effective therapies brought into common practice is that it either would compete with less effective treatments which are currently making the medical community substantial money, or similarly, because they haven’t found a way to charge enough money for the treatment. For example, it was found during research investigating the metabolic theory of cancer that fasting was useful in preventing epileptic seizures, and from this a ketogenic diet was fashioned, but which was found very hard to get included into the standard of care. This was because, ironically, it was too inexpensive! “The biggest problem [with implementation] today is trying to figure out how hospitals can reimburse trained ketogenic diet dietitians for their time.” (Pg158)
For all these reasons – and more – you will have wanted to purchase and have read this book.